search
A 38 year-old female, a smoker with hypothyroidism, diagnosed with Crohn's disease 5 years ago. The disease affected the terminal ileum. Medical therapy with Azatioprine was attempted, but she developed myelotoxicity. Methotrexate and anti-TNF were given, with no remission. She presented with bowel occlusion and a ileocecal resection was performed. Three months after the surgery she was still being treated with anti-TNF and developed a clinical relapse, requiring re admission due to a small bowel occlusion that was medically treated.
Due to an unsuccessful remission of the disease she was referred to our hospital for evaluation. A colonoscopy was performed revealing a normal mucosa but the anastomosis was stenotic and the small bowel could not be assessed.
An MRI was performed with T1 and T2 diffusion sequences plus oral mannitol, which provides correct distension of the bowel and the ideal exposure to study the entire wall. This study revealed 20 cm of terminal ileum with edema and mucosal hypercaptation and ulceration (VID 1) plus three additional stenotic segments (FIG 1).
This patient was counseled for tobacco cessation and a new surgical treatment. Due to the risk of relapse she prefers to maintain medical therapy with close follow up.
The patient is receiving anti-TNF and is attempting to quit tobacco. She has an average of 5 bowel movements per day and mild abdominal pain.
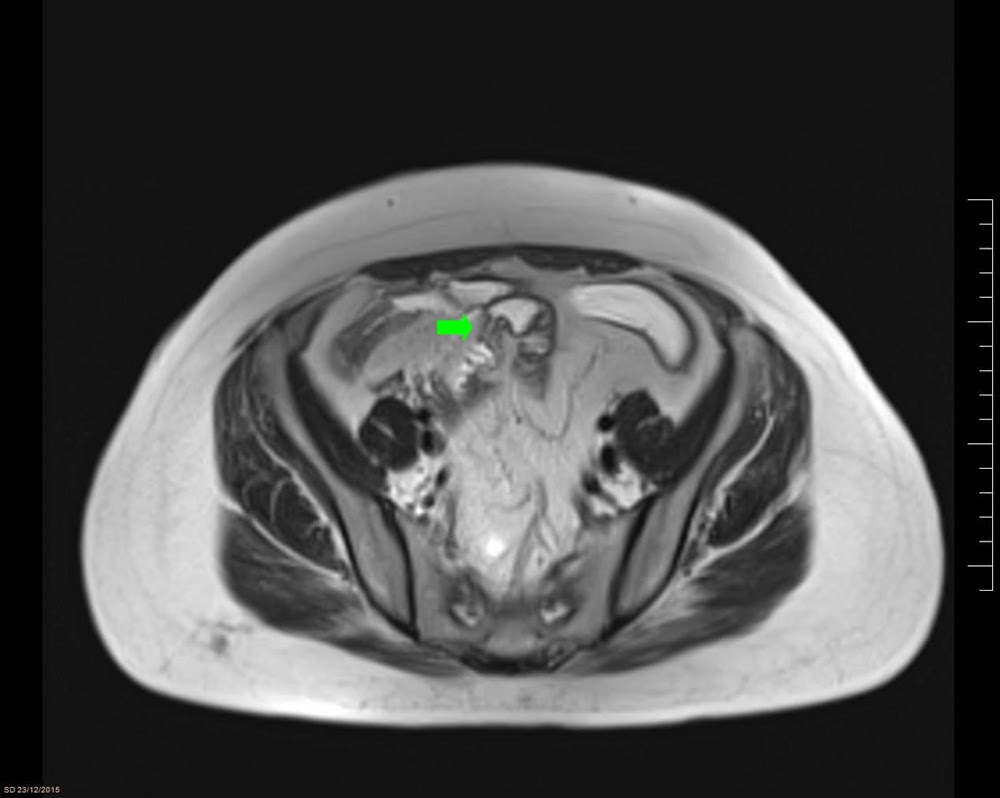 FIG 1. Stenotic small bowel
FIG 1. Stenotic small bowel
